Doctor Fauci and the Fear Factor – Quadrant Online
QUOTE
I had just received my copy of Robert Kennedy Jr’s latest book –
The Real Anthony Fauci – Bill Gates, Big Pharma, and the Global War on
Democracy and Public Health
[i] for my Christmas reading. It looked so delicious I read it
immediately, just couldn’t put it down. There are several things that I need
to say about it.
Firstly, it really is a must-read book. For anyone who has watched the COVID narrative evolve over the last two years much will come as no surprise, but the detail presented is staggering and some of it totally unexpected. Kennedy uncovers a whole new narrative that has been buried in plain sight. In order to formulate a response to the COVID issue, you really need to consider the entire big picture that Kennedy provides.
Secondly, one must always keep in mind that this book is from a true and
trusted Democrat, not someone who can be dismissed as a ‘right wing
nut job’, to quote one of the Left’s favourite contemptuous dismissals of
all and any who do not share their opinions and goals. But that also raises
an interesting sub-text, one that haunts the book. One of Kennedy’s motives
for writing appears to be to protect the legacy of his famous father and
uncles in the children’s services and AIDS fronts. Unfortunately for a
Democrat, that puts him on the wrong side of Dr Fauci who, as the book
documents, has a notorious history of exploitation
of vulnerable children (generally black and in orphanages) and AIDS
sufferers, the very people that Kennedy’s kin championed for years and which
helped build their political careers and reputations.
UNQUOTE
Quadrant is a decent source. Believe this article? I do.
Individuals with AIDS and HIV-positive asymptomatic individuals,
including pregnant women, have long been treated with toxic antiviral
drugs (AZT, Protease Inhibitors, as well as Nevirapine) that can cause
serious systemic injuries and even death. This is erroneously based on the
assumption that HIV is the cause of AIDS. Furthermore, the long-term
effects of these drugs on the composition of the human genomes have not
been determined. Prior to October of 1997, I believed that HIV was the
cause of AIDS based solely on the information that had been reported by
the United States Center for Diseases Control and Prevention (CDC) and the
AIDS establishment. However, my view was unquestionably changed when I
evaluated the medical evidence on the worldwide AIDS epidemic. My findings
clearly show: 1) The HIV-hypothesis is not supported by any medical fact
and AIDS is caused by agents and factors other than HIV. 2) The proponents
of the HIV-hypothesis have long overlooked crucial and essential medical
evidence that clearly describes the real causes of AIDS. 3) The results of
clinical studies on AZT, protease inhibitors, and nevirapine indicate that
these agents can cause severe systemic damage, AIDS, and death. However,
it is my opinion that the US Federal Drug Administration inappropriately
approved these drugs to be given to pregnant women and individuals with
serious health problems. My in-depth research findings are described in my
book "Get All the Facts: HIV Does Not Cause AIDS" in addition to my other
articles [1-7]. Below are examples that were selected from a large body of
evidence to illustrate my points.
Causes and pathogenesis of AIDS in drug users and homosexual men:
In the USA, about 90% of AIDS cases were male
homosexuals and
heterosexuals and homosexual drug users [8]. The
appearance of AIDS in the
USA and Europe in drug users and homosexuals in the late
1970’s and early
1980’s coincided with the synergistic actions of several
events. Briefly,
these include the spread of illicit drug use, especially
smoking crack
cocaine in 1970’s; the approval of glucocorticoids
aerosol by the US FDA
in 1976; the wide use of the glucocorticoid inhalers to
treat chronic
respiratory illnesses resulting from inhaling cocaine;
the wide use of
alkyl nitrites by homosexuals to facilitate anal sex in
1970’s; and the
wide use of corticosteroids to treat chronic
gastrointestinal tract
illness in homosexual men [1]. Furthermore, the approval
of antiviral
drugs (AZT and protease inhibitors) and the
corticosteroids by the US FDA
to treat patients with AIDS and asymptomatic patients
infected with HIV
has exacerbated the problem [1,8].
It has been stated that the use of alkyl nitrites to
relax the anal
muscle and facilitate anal sex permeated the gay life by
1977 [1].
Duesberg cited studies that show the significant use of
alkyl nitrites and
illicit drugs by homosexuals [9, 10]. These are: 1)
86.4% of 420
homosexual men attending clinics for sexually
transmitted diseases in New
York, Atlanta, and San Francisco reported that they
frequently used amyl-
and butyl nitrites as sexual stimulants and the
frequency of nitrite use
was proportional to the number of sexual partners; 2) a
total of 170 male
homosexuals from sexual disease clinics, including 50
with KS and
pneumonia, and 120 without AIDS were surveyed showing
50-60% had used
cocaine, 50-70% amphetamines, 40% marijuana, 10% heroin,
over 50% had also
used prescription drugs, about 80% had past or current
gonorrhea, 40-70%
had syphilis, 15% mononucleosis, 50% hepatitis, and 30%
parasitic
diarrhea; 3) A study of a group of 359 homosexual men in
San Francisco
reported in 1987 that 84% had used cocaine, 82% alkyl
nitrites, 64%
amphetamines, 51% methaqualone and 41% barbiturates; 4)
a total of 3916
self-identified American homosexual men were surveyed,
among which 83% had
used one, and about 60% of them used two or more drugs
with sexual
activities during the previous six months (similar drug
use has been
reported from European homosexuals at risk); and 6)
survey of homosexual
men from Boston, conducted between 1985 and 1988,
documented that among
206 HIV-positives, 92% had used nitrite inhalants,73%
cocaine, 39%
amphetamines, 29% lysergic acid in addition to six other
psychoactive
drugs as sexual stimulants.
The regular uses of alcohol, heroin, cocaine,
amphetamines, and alkyl
nitrite cause acute and chronic health problems of the
nervous system,
respiratory system, cardiovascular system, kidneys and
other tissues in
these individuals. The majority of these health problems
are typically
diagnosed as “idiopathic” and currently treated with
high doses of
glucocorticoids and/or cytotoxic drugs. In addition,
some homosexual men
use rectal glucocorticoids as a treatment for chronic
injuries [1, 8].
The treatment of a patient with prednisone at 60 mg per
day for about
three months can actually cause AIDS [1]. This treatment
and doses often
given to patients suffering from lung fibrosis,
thrombocytopenia, or other
chemically induced chronic illnesses. For example, Fauci
et al. described
the treatment for patient with lung fibrosis as follows:
“A trial of oral
prednisone is begun at a dose of 1mg/kg daily and
continued for about 8
weeks. Should the disease not respond or be progressive,
additional
immunosuppression with cyclophosphomide should be
considered. The
objective is to reduce the white blood cell count to
approximately half
the normal baseline value, causing a distinct drop in
the total lymphocyte
count. However, a minimum count of 1000 PMNs/µL should
be maintained” [8,
page 1463]. At this dose levels, the CD4+T cells count
in the peripheral
blood of the treated individual is expected to be
<300/µL which meets
the definition for AIDS set by the US Center For
Diseases Control and
Prevention (CDC).
The following is HIV-negative drug user woman who
developed AIDS
following a few months of treatment with
immunossuprassants. A 33-year-old
previously healthy female developed acute bilateral
pulmonary infiltrates
after 18 hours of intense rock cocaine (crack) smoking.
Ten months later,
she developed progressive dyspnea and interstitial
pneumonia. She was
unsuccessfully treated with high doses of prednisone (1
mg/kg/day for
eight weeks) followed by a trial of cyclophosphamide.
She died due to
respiratory failure with a superimposed mycobacterial
infection. The time
from her first admission to the hospital with
interstitial pneumonia and
her death with AIDS was about 21 months [11].
In addition, I reviewed 7 selected studies that
included 736 patients
(97% of them were homosexual or bisexual men) who were
infected with HIV
and/or had AIDS. I found that these individuals suffered
from extensive
rectal and gastrointestinal problems that dictate the
chronic use of
therapeutic rectal corticosteroids [1].
Review of the medical literature revealed that the
short and the long
term use of glucocorticoids at therapeutic doses,
resulted in a variety of
effects on the immune system that range from a transient
reduction in T
cells count in peripheral blood to the development of
full blown AIDS. In
1975 and 1976, Fauci and Fauci et al. described in
detail the effects of
corticosteroids on the immune system [12,13]. These
effects resemble the
immune abnormalities that are found in patients
suffering from AIDS or
Idiopathic CD4 T cells lymphocytopnea (ICL), which are
also described by
Fauci et al. in 1998 [8]. For instance, in 1976, Fauci
et al. stated that
“we have reviewed many aspects of the host defenses that
are altered by
corticosteroids, and the combined effects of these
changes must be
considered in trying to understand the relation between
corticosteroids
and infections. Since the defect with corticosteroids is
broad, it is not
surprising that many types of infections seem to occur
more often in
patients treated with corticosteroids. Of the bacterial
infections,
staphylococcal and Gram-negative infections, as well as
tuberculosis and
Listeria infections, probably occur most often. Certain
types of viral,
fungal, and parasitic infections also occur often.
Studies of bronchial
aerosols showed that with higher doses of steroid in the
aerosol, Candida
infections of the larynx and pharynx occurred more
often” [13].
The reversal of CD4+ T cells depletion in the
peripheral blood was
reported in HIV-positive homosexual men after the
termination of their
treatment with glucocorticoids [14, 15]. Sharpstone et
al. reported that
eight HIV-positive males with inflammatory bowel disease
who used rectal
steroid preparation had a decline in their CD4+ T cells
at a rate of 85
cells/µL per year [14]. Four of them underwent
coloectomy that eliminated
the need for the steroid and their CD4+ T cells
increased 4 cells/µL per
year. Eight HIV-positive men used as match control who
did not have
surgery continued to have a decline of 47 cells/µL per
year as the result
of the use of rectal steroid. In addition, investigators
from George
Washington University and the National Institutes of
Health reported a
case of HIV-positive homosexual man with ulcerative
colitis who developed
a severe reduction in CD4+ T cells counts following 9
days treatment with
corticosteroids and the depletion in CD4+ T cells number
was reversed
following the cessation of the treatment [15]. Briefly,
approximately 3
weeks prior to surgery for ulcerative colitis that was
unresponsive to
corticosteroids, the patient's CD4+ T cell count was 930
cells/µL of blood
and the count fell to 313 cells/µL within 10 days of
treatment with
corticosteroids. Five days postoperatively, the patient
become
asymptomatic and was discharged on tapering prednisone
without the use of
antiretroviral agents. After surgery, the patient's CD4+
T cells counts
progressively rose. The CD4+ T cells counts were 622
cells/µL and 843
cells/µL at 3 and 6 weeks following the operation,
respectively.
Kaposi’s sarcoma (KS), an AIDS-indicator disease also
developed in
HIV-negative patients chronically treated with
glucocorticoids [1, 16].
For example, KS developed eight months after initiation
of prednisone
treatment (40 mg per day for three months) in
HIV-negative man. He also
had lymphocytopenia (896/µL), reduction of T4 (CD4+)
cells (215/µL), and
T4/ T8 ratio of 0.7. [16]. In addition, there are many
cases who
developed KS following treatment with glucocorticoids
and they had
reversal of their KS after the termination of the
treatment [1].
My investigation also revealed that the majority of
AIDS patients
suffer from metabolic and endocrine abnormalities [1].
The high
prevalence of adrenal insufficiency observed among AIDS
patients provides
very strong evidence that AIDS in these patients is
caused by the use of
corticosteroids. Fauci et al. stated that endocrine and
metabolic
abnormalities are frequently seen in HIV-infected
individuals and most HIV
-infected individuals studied at autopsy had involvement
of adrenal glands
[8]. The most common abnormality seen in HIV infected
individuals is
hyponatremia, seen in up to 30 percents of patients.
They also stated in
the same book that the presence of a low sodium level
combined with a high
serum potassium level in a patient should alert one to
the possibility of
adrenal insufficiency and adrenocortical insufficiency
as seen following
prolonged administration of excess glucocorticoids [8].
However; the use
of corticosteroids by AIDS patients was not considered
by Fauci and his
colleagues.
The HIV-hypothesis states that HIV cause AIDS by
killing the CD4+ T
cells directly or indirectly [8]. It appears that there
is no scientific
evidence to show that HIV can kill infected T4 cells
(CD4+ T cells) in
vitro or in vivo. In addition, the abnormalities in the
immune system of
patients with AIDS are not restricted to the reduction
of T4 cells as
predicted by the HIV-hypothesis. Hoxie et al. observed
no evidence of
death in T cells infected with HIV in tissue culture
[17]. These cells
continued to produce virus particles for more than four
months after
inoculation with the virus. Many reports described the
changes in the
lymph nodes of patients infected with HIV and these
changes range from
extensive cellular hyperplasia of T and B lymphocytes
and the supporting
stroma to severe atrophy of the glands. Changes in the
lymph nodes of 505
HIV-positive patients who were asymptomatic or had AIDS
demonstrate three
distinct stages [1]. These are hyperplasia (245
patients), atrophy (117
patients), and mixed stage (172 patients). The presence
of hyperplasia in
the infected lymph nodes contradicts the HIV-hypothesis
which states HIV
destroys infected T cells [8].
The proponents of the HIV-hypothesis provide further
elucidation.
Muro-Cacho, Pantaleo, and, Fauci examined 29
HIV-positive lymph nodes and
found twelve of these lymph nodes with follicular
hyperplasia and
extensive germinal centers, five with follicular
hyperplasia mixed with
follicular involution, twelve lymph nodes with a mixture
of follicular
involution and lymphocyte depletion, and five lymph
nodes with lymphocyte
depletion [18]. They stated that “apoptosis was not
restricted only to
CD4+ T cells; both B cells and CD8+ T cells were found
to undergo
apoptosis. They also stated that the increased intensity
of the apoptotic
phenomenon in HIV infection is caused by the general
state of immune
activation, and is independent of the progression of HIV
activities and
the levels of viral load”. HIV provirus was also found
in CD4+ T cells,
CD8+ T cells, and B cells lymphocytes in the lymph nodes
of HIV infected
patients and its ability to infect cells is not
restricted to cells that
have CD4 receptor as predicted by the HIV-hypothesis
[1].
The changes in the lymph nodes described above are
not unique to HIV-
infected individuals but also were described in
HIV-negative patients in
risk groups. The lymph nodes from 215 HIV-negative
homosexual and drug
users men showed hyperplasia in 187 patients and atrophy
in 28 patients,
and 15 lymph nodes showed Kaposi’s sarcoma and lymphoma
[1]. US CDC
considers these changes as AIDS-indicator illnesses, yet
the subjects were
HIV-negative.
In addition to the information presented above that
demonstrates the
invalidity of the HIV-hypothesis, the rates of T cells
infection by HIV,
and the rates of the thymus and the lymphoid tissue
regeneration also
conflict with the HIV-hypothesis. Duesberg stated that
HIV infects on the
average only 0.1% (1 out of 500 to 3000) of T-cells in
AIDS patients, and
at least 3% of all T-cells are regenerated during the
two days it takes a
retrovirus to infect a cell [9]. HIV could never kill
enough T cells to
cause immunodeficiency. Thus, even if HIV killed every
infected T cell, it
could deplete T cells only at 1/30 of their normal rate
of regeneration,
not considering activated regeneration. Gallo agreed
with Duesberg that 1
in 10000 T cells are infected with HIV [19]. Baltimore
and Feinberg also
stated that, in the late stage of AIDS disease, HIV
infects 1 in 100 CD4+
T cells or 1 in 400 mononuclear cells [20]. Furthermore,
Al-Bayati et al.
found that the rates of regeneration in the damaged
thymus and lymphoid
tissue of mice treated with a lymphotoxic agent
(vanadate) are very high
[21]. A total of 120 mice were treated with metavanadate
solution (15.5
mg/kg). Severe necrosis in the thymus of treated mice
was observed at 2
days following treatment and the thymus healed
completely in about 10
days.
Some studies show increases in CD4+ T cells in
HIV-positive
individual after treatment with the antiviral drugs [1].
This information
was interpreted as a good response to the medications.
On the contrary,
the elevation of T cells is not a good response in these
conditions, but
rather, it indicates severe tissue damage and infection.
This explains the
death of the patients following treatment with these
drugs. For example,
the CD4+ T cells were also increased following the
treatment of HIV-
negative nurses with AZT who took AZT as a prophylactic.
They developed
severe symptoms following 3 weeks of treatment with AZT
[1]. In addition
to the failure of the antiviral drugs, AIDS patients
suffering from immune
deficiency are treated with glucocorticoids [8]. This
practice is not
supported by any known biomedical mechanism of action.
The causes of AIDS in infants and children:
In the United States of America, ninety percent of
infants and
children who developed AIDS had mothers who were drug
users [8]. The
prevalence of cocaine use among pregnant women in the
USA is relatively
high as shown by countless studies [1,8].
Cocaine-positive urine was found
in 15.3% of 411 pregnant women surveyed in hospitals at
the time of
delivery. During 1993, 12.8% (361 of 2810) of all live
singleton infants
born at Harem Hospital in New York were identified as
cocaine exposed. The
impact of illicit drug and alcohol abuse during
pregnancy on infant health
is extremely serious. Nine studies that included 1,295
drug-using mothers
and 4,293 nonusers showed that cocaine use during
pregnancy led to a high
prevalence of premature births and low birth weights
[1].
A mother expected to have a premature birth is
treated with
glucocorticoids prior to delivery to facilitate the
development of the
lungs and to reduce the incidence of necrotizing
enterocolitis in a
premature infant. Drug exposed infants usually have
serious health
problems that are treated with glucocorticoids [1]. In
addition, the
natural cortisol levels in plasma and urine of the
cocaine-exposed preterm
neonates was also found to be significantly higher than
in normal infants
[22]. Therapeutic glucocorticoids and endogenous
cortisol can cause severe
reduction in T cells and B cells numbers and their
functions. The long-
term use of corticosteroids at the therapeutic levels
causes atrophy of
the thymus and lymphoid tissue of infants, children, and
adults and
increases the incidence of infections [1, 8, 23].
The histology of the thymus of HIV-infected infants
and children
showed changes such as atrophy of the lymphoid tissue,
Hassall's
corpuscles, and connective tissue. These changes are
consistent with those
observed in the lymphoid organs of HIV-negative
individuals suffering from
severe malnutrition or treated with high doses of
corticosteroids.
Moreover, HIV-positive infants and children who died
with AIDS suffered
from opportunistic infections (tuberculosis, fungal,
yeast, and viral
infections) similar to those reported in HIV-negative
infants and children
suffering from malnutrition or treated with high doses
of corticosteroids
[1, 8, 23, 24]. However, the proponents of the
HIV-hypothesis have not
considered corticosteroids as a factor of causing AIDS
in the risk groups
who are receiving high doses of these agents. On the
contrary,
corticosteroids are used to treat people with AIDS who
suffer from
tuberculosis, thrombocytopenia, peripheral neuropathy,
lung fibrosis, and
other chronic diseases. This approach is unscientific
and should be
evaluated.
Anthony Fauci and the proponents of the
HIV-hypothesis have long been
aware of the use of illicit drugs among pregnant women
and the impact of
drug use on the health of mothers and their infants as
shown in their
literature. For instance, Fauci et al. explained the
impact of illicit
drugs on the pregnant mothers and their infants as
follows: women who
abuse cocaine have reported major derangement in
menstrual cycle function,
including galactorrhea, amenorrhea, and infertility.
Chronic cocaine abuse
may cause persistent hyperprolactinemia as a consequence
of cocaine-
induced disorders of dopaminergic regulation of
prolactin secretion by the
pituitary. Cocaine abuse, particularly the smoking of
crack by pregnant
women, has been implicated as causing an increased risk
of congenital
malformations and prenatal cardiovascular diseases in
the infants. Cocaine
abuse per se is probably not the sole reason for these
prenatal disorders
since many problems associated with maternal cocaine
abuse, including poor
nutrition and health care status as well as polydrug
abuse, also
contribute to the risk of prenatal diseases [8].
In addition, Fauci et al. stated that a special case
of opiate
withdrawal is seen in the newborn passively addicted by
the mother's drug
misuse during pregnancy. Some level of addiction
develops in 50 to 90
percent of children of heroin-dependent mothers. The
syndrome consists of
irritability, crying, and tremor in 80%; increased
reflexes, increased
respiratory rate, diarrhea, and hyperactivity in 60%;
vomiting in 40%; and
sneezing, yawning, and hiccupping in 30%. The child
usually has a low
birth weight and may be otherwise unremarkable until the
second day, when
symptoms are likely to begin [8].
O'Shea et al. evaluated the outcome of pregnancy of
95 HIV-positive
pregnant women and found that there was little variation
in plasma viral
load occurred during pregnancy. However, there was an
association between
viral load and prematurity; the mean gestation at
delivery decreasing by
1.3 weeks for every 10-fold increase in maternal HIV RNA
[25]. We know
that HIV does not induce labor but premature delivery is
a good indicator
for drug use as described above and in Fauci's book and
my book [1,8]. The
findings of this study and others indicate that HIV is a
good marker for
drug use, practicing unsafe sex, in addition to poor
hygiene.
I reviewed the designs and the results of numerous
AZT and protease
inhibitors clinical trials and found that AZT and
protease inhibitors are
very toxic drugs and the conclusions of these studies do
not support the
claims that these drugs can be used to cure people with
AIDS [1]. On the
contrary, AZT causes severe bone marrow depression and
reduces white blood
cells counts including T cells. It is very toxic to the
stem cells in bone
marrow (the source of T and B lymphocytes) and to fast
growing tissues
such as embryonic and fetal tissues. For example, Fischl
et al. treated
145 AIDS patients treated with AZT for up to 24 weeks.
The CD4+ T cell
counts of these patients were reduced from baseline of
66/µL to 37/µL
[26]. Some patients felt very sick and treatment was
terminated early.
In a second study, Fischl et al. gave AZT to 524
subjects who had a
first episode of Pneumocystis carinii pneumonia [27].
These subjects
received AZT in either a dose of 250 mg taken orally
every four hours
(n=262) or a dose of 200 mg taken orally every four
hours for four weeks
and thereafter 100 mg taken every four hours (n=262). In
this study,
additional AIDS-defining opportunistic infections
developed in 429
subjects (82%) in the AZT treated groups. Furthermore,
the neutrophil
counts declined to less than 34% of baseline in 230
subjects; the
hemoglobin levels declined to less than 66% of baseline
in 178 subjects;
and one hundred thirty-four subjects received red-cell
transfusions. One
hundred eighty-three subjects (35%) were withdrawn from
AZT therapy
because of toxic reactions such as severe anemia and
neutropenia. At 24
months of treatment, the mortality rates were 66% and
73% in the low and
standard AZT doses, respectively.
Besides, the following is a list of some of the
serious adverse
reactions to AZT that have been reported in infants,
children, and adults
as stated in the drug information book for physicians
and other databases
to illustrate the danger of AZT [1, 8, 23]. These
reactions may include,
neutropenia, granulocytopenia, anemia, thrombocytopenia,
myopathy and
myositis, hepatomegaly with steatosis, hepatitis,
pancreatitis, lactic
acidosis, sensitization reactions, hyperbilirubinemia,
vasculitis,
abdominal pain, back pain, body odor, chest pain,
chills, edema of the
lip, fever, flu syndrome, hyperalgesia, syncope,
vasodilation, bleeding
gums, constipation, diarrhea, dysphagia, edema of the
tongue, eructation,
flatulence, mouth ulcer, rectal hemorrhage,
lymphadenopathy, arthralgia,
muscle spasm, tremor, twitch, anxiety, confusion,
depression, dizziness,
emotional lability, loss of mental acuity, nervousness,
paresthesia,
somnolence, vertigo, cough, dyspnea, epistaxis,
hoarseness, pharyngitis,
rhinitis, sinusitis, acne, changes in skin and nail
pigmentation,
pruritus, rash, sweat, urticaria, amblyopia, hearing
loss, photophobia,
taste perversion, dysuria, polyuria, urinary frequency,
and urinary
hesitancy.
The adverse reactions of the second drugs (Nevirapine)
that have also
been given to HIV-pregnant women may include severe and
life-threatening
skin reactions (stevens-johnson syndrome, toxic
epidermal necrolysis),
severe and life-threatening hepatotoxicity, skin rash,
maculopapular
erythematous cutaneous eruptions, fever, nausea,
headache, and
granulocytopenia [23]. In addition, the safety profile
of this drug in the
neonates has not been established.
The information presented above describing the
toxicities of AZT and
nevirapine tells the horrifying stories about the
suffering of pregnant
women, infants, and children who are given these toxins
based on a false
assumption that HIV is a killer virus. Some of these
people are forced to
ingest these toxins. This is heartbreaking!
Causes and pathogenesis of AIDS in hemophiliacs:
The medical evidence shows that AIDS in hemophiliac
patients is
caused by the treatment with immunosuppressive agents
(cyclophosphamide
and/or glucocorticoids) to prevent the development of
antibodies to
factors VIII and XI. Fauci et al. also described the
development of
antibodies against factors VIII and IX and the use of
corticosteroids in
the hemophilia patients [8]. Patients with severe
hemophilia usually have
serious chronic joint problems resulting from bleeding
inside the joints
and this is also treated with glucocorticoids. Low CD4+
T cells counts
have been observed in both HIV- negative and
HIV-positive hemophiliac
patients. Duseberg presented the results of 17 studies
showing that a
total of 717 hemophiliac patients had T4/T8 ratios less
than or equal to
one and 46% of them (329 patients) were HIV-negative
[9].
Causes and pathogenesis of AIDS in organ transplant
and/or blood
transfusion patients:
As of January 1, 1997, the number of patients in the
USA who received
blood transfusions, blood components or tissues then
subsequently
developed AIDS was 7,888 [8]. Adverse reactions to blood
transfusion have
been frequently reported and the standard treatment used
to prevent or
cure these reactions is glucocorticoid as stated by
Fauci et al. [8]. For
example, the risk of getting an allergic reaction from a
blood transfusion
is 1-4 per 100. The risk for delayed hemolytic reaction
is 1 per 1,500. In
contrast, the risk of infection with HIV from blood
transfusion is 1 per
490,000 [8]. However, immune suppression as a result of
the use of
glucocorticoids in these patients was not investigated.
Furthermore,
glucocorticoids and other immunosuppressive agents are
also used to
prevent tissue rejection in organ transplant patients.
The complications
from these treatments and the list of opportunistic
diseases are also
described by Fauci et al [8]. The list of opportunistic
diseases in organ
transplant patients receiving immunosuppressive agents
is identical to the
list of opportunistic diseases listed in people with
AIDS [8].
Causes and pathogenesis of AIDS in Africa:
As of November 1996, the number of AIDS cases
reported in Africa by
the World Health Organization was 553,291 [8]. Severe
malnutrition has
been very well known to cause immune dysfunction and
other serious health
effects. It should be considered in the differential
diagnosis in HIV-
infected patients with AIDS and suffering from severe
malnutrition before
implicating HIV as the cause of AIDS in Africa. Actually
the finding of
atrophy of lymphoid tissue in people suffering from
malnutrition was
observed as early as 1925. For example, Jackson’s review
on this topic in
1925 noted that many investigators had found a
pronounced tendency of
atrophy of lymphoid tissue in all conditions of
malnutrition. Thymus
weight was exquisitely sensitive to malnutrition and was
earlier
designated as the “barometer of nutrition” [28].
The functions of the immune system, especially the
cellular immunity,
are impaired in malnutrition cases. The severity of the
impairment is
dependent on the degree of malnutrition in both human
and animal. The size
of the thymus of 42 malnourished children was reduced by
90% as compared
with the size in the normal children of the same age
[29]. In a second
study involving 110 malnourished children, the thymic
area was found to be
20% of the size in healthy children [30]. The results of
autopsy of 118
malnourished children showed: 1) both thymus and
peripheral lymphoid
tissues were reduced in bulk in protein-calorie
malnutrition (PCM), this
reduction being disproportionately greater than the loss
of body weight;
and 2) severe thymic atrophy was presented in 70% of
marasmus cases and
85% of Kwashiorkor cases and 59.3% of the children had
marasmic and
Kwashiorkor symptoms [31]. Fakhir et al. evaluated 100
severely
malnourished children and found that these children had
a significant
reduction in the absolute lymphocytes counts, T cells
counts, and in the
skin reaction to dinitrochlorobenzene [32]. The
lymphocyte functions of 30
black children with PCM as assessed by the delayed
hypersensitivity
reaction and morphology of lymphocyte transformation
were found to be
impaired and serum cortisol level was elevated [33]. The
functions of
lymphocytes and cortisol levels in these patients were
returned to normal
after 30 days of feeding.
Atrophy in the lymphoid organs in malnourished people
is caused by
increased levels of cortisol as well as by protein and
vitamin deficiency.
The reduction in the thymus and the lymphoid tissue size
and the reduction
in the functions of the immune system of malnourished
children and animals
were reversed after proper feeding. For example, the
size of the thymus
increased from 20% of normal in a malnourished child to
107% of normal
following 9 weeks of proper feeding [30]. The levels of
endogenous
cortisol in plasma and urine have been found to be
abnormally elevated in
malnourished patients as shown by studies included 159
malnourished
children and 148 AIDS patients [1].
The incidence of starvation, parasitic diseases,
septicemia, and low
birth weight are very high in Africa and other
developing countries as
shown in eleven studies that include the prevalence of
malnutrition and
diseases in 1,425 infants and 5,834 children surveyed in
nine countries
[1]. For example, the mortality rate among 299 severely
malnourished
children in Zambia was 25.8% [34]. Pneumonia and
diarrhea were the major
causes of death. In India, 49% of 183 cases of
lymphadenopathy in
children were found to be due to tuberculosis [35].
The prevalence of KS and lymphoma, lymphadenitis, and
tuberculosis in
Africa are similar to those reported in the male
homosexuals AIDS patients
in US and Europe and even higher [1]. However, AIDS in
Africa occurs
almost equally in males and females because starvation
affects both sexes
equally. Sibanda and Stanczuk reviewed all lymph nodes
histopathology
reports of lymph nodes biopsies submitted to the
Histopathology unit in
Harare, Zimbabwe, in the period of January 1988 to June
1990. They found
that the commonest diseases in the 2,194 lymph node
specimens were: non-
specific hyperplasia (33%), tuberculous lymphadenitis
(27%); metastases
(12%), Kaposi’s sarcoma (9%); and lymphomas (7%).
Kaposi’s sarcoma (KS)
involving the lymph nodes was reported in 176 (9%) of
the lymph nodes
[36]. In children, the prevalence of KS was higher in
children under 5
years than in 6-15 year bracket. In adults,
approximately two thirds (65%)
of all patients with KS were aged between 20 and 40
years.
The study of Fawzi et al. in Tanzania clearly
demonstrated that HIV
is a harmless virus. Feeding HIV-positive malnourished
pregnant women
proper nutrition reversed the impairments of the immune
system functions.
This measure also improved the outcome of their
pregnancy [37]. They gave
1,075 HIV-infected pregnant women between 12 and 27
weeks' gestation
vitamin A (n=269), multivitamins excluding vitamin A
(n=269),
multivitamins including vitamin A (n=270), or a placebo
(n=267). All T-
cells subsets (CD4+, CD8+, and CD3+) increased in all
treatment groups
from baseline levels during pregnancy and 6 weeks
following delivery.
There was a significantly larger increase in the CD4+ T
cell counts and
percentage of CD4+ T cells among women assigned
multivitamins. The mean
increases between baseline and 6 weeks postpartum were
167 cells/µL and
112 cells/µL among women on multivitamins and those on
no vitamins,
respectively. Vitamin supplementation also decreased the
risk of low birth
weight (<2500 g) by 44%, severe preterm birth (<34 weeks
of
gestation) by 39% and small size for gestational age at
birth by 43%.
Summary of findings:
1) HIV is a harmless virus, both in vivo and in
vitro. The HIV-
hypothesis is not supported.
2) AIDS in drug users and homosexuals in the U.S. and
in Europe
results from heavy ancillary use of glucocorticoids and
other
immunosuppressive agents. Physicians prescribe these
drugs to treat a wide
range of chronic illnesses of the respiratory and
gastrointestinal
systems, and other organs.
3) The appearance of AIDS in the U.S. and Europe
coincided with the
approval of glucocorticoid aerosol use in 1976, the
introduction of crack
cocaine, the use of heroin by inhalation, and the use of
alkyl nitrites by
homosexuals to enhance anal sex.
4) AIDS in hemophiliacs relates to the use of
corticosteroids and
other immunosuppressive agents to prevent development of
antibodies for
factors VIII and IX, and used to treat other chronic
illnesses such as
joint disease.
5) AIDS in people receiving blood and/or tissue
follows use of
glucocorticoids to prevent transfusion and tissue
rejection, and to treat
other illnesses.
6) AIDS in infants and children is caused by their
exposure to drugs
and corticosteroids in utero, and to corticosteroids
used after birth to
treat their chronic illnesses.
7) AIDS in Africa results from malnutrition, the
consequent release
of endogenous cortisol, and opportunistic diseases.
Atrophy in the thymus
and lymphoid tissue in people suffering from
malnutrition has been known
since 1925; malnutrition also impairs T cells function.
Feeding an
adequate diet reverses these changes. It cures AIDS!
Thymus size in
malnourished children increased from 20% of normal to
107% of normal,
after nine weeks of feeding.
8) Kaposi's sarcoma (KS) and lymphoma result from the
use of steroids
and drugs, and the release of endogenous cortisol. They
are not caused by
a slow virus. Stopping treatment with immunosuppressive
agents prior to
metastasis reverses KS in some cases.
9) The medications currently used to treat patients
with AIDS, such
as AZT, protease inhibitors, and glucocorticoids are
highly toxic. They
can cause AIDS in asymptomatic patients; they worsen the
condition of AIDS
patients and even lead to their death. These drugs have
no therapeutic
value; their use should stop forthwith.
10) Damage to the immune system is rapidly reversible
after removal
of the true insulting agent or treatment of the true
causes. Examples: a)
The CD4+ T cells of 1,075 HIV-positive pregnant women
increased from
426/uL to 596/uL in six months on a balanced diet. This
also improved the
outcome of their pregnancies; and b) In HIV-positive
homosexuals, stopping
treatment with glucocorticoids reversed a fall in CD4+ T
cells.
Urgent actions are needed to correct the problem:
I hope that the medical evidence presented in this
article along with
the cited references will alert you to the facts that
unfortunately we are
moving in the wrong direction concerning the war on
AIDS. It is
incredibly difficult to imagine that A. Fauci, the
director of the AIDS
program at the National Institute of Health, has spent
billions of dollars
to find a cure for AIDS, yet the solutions for the AIDS
crisis are
presented in his very own publications. We have a large
body of medical
evidence that clearly shows HIV does not cause AIDS. I
urge each and every
government, including all individuals, to review the
evidence. The AIDS
establishment's unscientific, costly, and risky approach
needs to be re-
examined to save the world population from an imminent
tragic consequences
from the wide use of toxic drugs and to save important
resources.
Implementing effective preventives measures can solve
the problem of
AIDS. These include: 1) prevent the causes of AIDS by
educating the
public about the toxic effects of the illicit drugs and
alcohol; 2) limit
the use of glucocorticoids in the treatment of chronic
health conditions
and in the treatment of people with AIDS; 3) monitor the
levels of CD4+ T
cells and CD8+ T cells in the blood of patients who are
receiving medium
or high therapeutic doses of glucocorticoids for a
significant time; 4)
discontinue the treatment of patients with AIDS and
asymptomatic HIV-
positive patients with AZT and protease inhibitors
immediately since these
are very toxic medications and have no therapeutic
values; 5) provide
proper clinical support and nutrition to patients with
AIDS based on their
medical needs
References
[1] Al-Bayati, MA. Get All The Facts: HIV does not
cause AIDS. Toxi-
Health International, Dixon, CA 1999 [http://www.toxi-health.com].
[2] Al-Bayati, MA. The Real Cause of AIDS. Mecola's
health
newsletter, Issue 236, July 11, 2001
[http://www.mercola.com/2001/jul/11/aids3.htm].
[3] Al-Bayati, MA. Is there proof that HIV-positive
persons
consistently develop illnesses that are rare or never
occur in HIV
negative persons? Virusmyth.net, September 2001
[http://www.virusmyth.net/aids/data/mabcdc.htm].
[4] Al-Bayati, MA. HIV Does Not Cause AIDS. The
British Medical
Journal, January 30, 2002
[http://bmj.com/cgi/eletters/324/7331/237].
[5] Al-Bayati, MA. Keep The Dentist Working: HIV Does
Not Cause AIDS.
The British Medical Journal, March 15, 2002
[http://bmj.com/cgi/eletters/324/7337/564#20541].
[6] Al-Bayati, MA. AIDS in Africa is caused by
Starvation and
Medications. The British Medical Journal, March 7, 2002
[http://bmj.com/cgi/eletters/324/7335/446/a#20389].
[7] Al-Bayati, MA, Flores JJ, Hosbein LM, Maggiore C.
Resolution of
AIDS in HIV Positive Patients: A Clinical Study of
Non-HIV Causes and
Treatments for AIDS Illnesses, 2000 [www.aliveandwell.org/index.php?
page=study].
[8] Fauci AS, Braunwald E, Isslbacher KJ, Wilson, JD,
Martin JB,
Kasper DL, Hauser SL, Longo DL. Harrison's Principles of
Internal
Medicine. McGraw-Hill Companies, Inc. New York USA, ed.
14, 1998
[9] Duesberg PH. AIDS Acquired by drug consumption
and other
noncontagious Risk Factors. Pharmac. Ther. 1992; 55:
201-277
[10] Duesberg PH. The role of drugs in the origin of
AIDS. Biomed
Pharmacother 1992; 46:3-15
[11] O’Donnell AE, Mappin FG, Sebo TJ, Tazelaar H.:
Interstitial
pneumonitis associated with “crack” cocaine abuse. Chest
100(4):1155-7,
1991
[12] Fauci AS. Mechanisms of Corticosteroid Action on
lymphocyte
subpopulations I. Redistribution of circulating T and B
lymphocytes to the
bone marrow. Immunology 1975; 28: 669-679
[13] Fauci AS, Dale DC, Balow JE. Glucocorticosteroid
therapy:
Mechanisms of Action and Clinical Considerations. Annals
of Internal
Medicine 1976; 84:304-15
[14] Srpstone DR, Duggal A, Gazzard BG. Inflammatory
bowel disease in
individuals seropositive for the human immunodeficiency
virus. Eur. J.
Gastroentrol. Hepatol 1996; 8:575-8
[15] Silver S, Wahl SM, Orkin BA, Orenstein JM.
Changes in
circulating levels of HIV, CD4, and tissue expression of
HIV in a patient
with recent-onset ulcerative colitis treated by surgery,
Case report.
Journal of Human Virology 1999; 2:52-7
[16] Schottstaedt MW, Hurd ER, Stone MJ. Kaposi’s
sarcoma in
rheumatoid arthritis. Am J Med 1987; 82:1021-6
[17] Hoxie JA, Haggarty BS, Rackowski JL, Pillsury N,
Levy JA.
Persistent Noncytopathic Infection of Normal Human T
lymphocytes with
AIDS-Associated Retrovirus. Science 1985;
229(4720):1400.
[18] Muro-Cacho CA, Pantaleo G, Fauci AS. Analysis of
apoptosis in
lymph nodes of HIV-infected persons. Intensity of
apoptosis correlates
with the general state of activation of the lymphoid
tissue and not with
stage of disease or viral burden. J. Immunol 1995;
154:5555-66
[19] Booth W. A rebel without a cause of AIDS.
Science 1988;
239(4847):1485-1488
[20] Baltimore D, Feinberg MB. HIV revealed: Toward a
natural
history of infection. The New England Journal of
Medicine 1989; 321:1673-4
[21] Al-Bayati MA, Culbertson RM, Schreider JP,
Rosenblatt LS, Raabe
O.G. The Lymphotoxic Action of Vanadate. Journal of
Environmental
Toxicology and Oncology 1992; 11:19-27
[22] Scafidi FA, Field TM, Wheeden A, et al.
Cocaine-exposed preterm
neonates show Behavioral and hormonal differences.
Pediatrics 97(6 Pt
1):851-5, 1996
[23] USPDI. Drug Information for the health care
professional. Volume
1, 21st Edition, Published & Distributed by Micromedex,
Englewood, Co,
USA
[24] Drut R, Anderson V, Greco MA, et al.:
Opportunistic infections
in pediatric HIV Infection: a study of 74 autopsy cases
from Latin
America. The Latin American AIDS pathology study group.
Pediatr Pathol Lab
Med 17(4):569-76, 1997
[25] O'Shea S, Newell ML, Dunn DT, et al.: Maternal
viral load, CD4
cell count and vertical transmission of HIV-1. J. Med.
Virol 54(2):113-7,
1998
[26] Fischl MA, Richman DD, Grieco MH, et al.: The
efficacy of
Azidothymmidine (AZT) in the treatment of patients with
AIDS and AIDS-
related complex. A double-blind, Placebo-Controlled
Trial. The New England
Journal of Medicine. Volume 317, number 4 (185-191),
1987
[27] Fischl, MA, Corette BP, Pettinelli C, et al. A
randomized
controlled trial of a reduced daily dose of zidovudine
in patients with
the acquired immunodeficiency syndrome. The New England
Journal of
Medicine 1990; 323:1009-14
[28] Woodruff JF. Thymolymphatic deficiency and
depression of cell-
mediated immunity in protein-calorie malnutrition.
Lancet 1972;
1(7741):92-3.
[29] Parent G, Chevalier P, Zalles L, Sevilla R,
Bustos M, Dhenin JM,
Jambson B. In vitro lymphocyte-differentiating effects
of thymulin (Zn-
FTS) on lymphocyte subpopulation of severely
malnourished children. Am.
J. Clin. Nutr 1994; 60:274-8
[30] Chevalier P, Sevilla R, Sejas E, zalles L,
Belmonte G, Parent,
G. Immune recovery of malnourished children takes longer
than nutritional
recovery: implications for treatment and discharge. J.
Trop Perdiatr 1998;
44:304-7
[31] Schonland M. Depression of immunity in
protein-calorie
malnutrition:a post-mortem study. J. Trop Pediatr
Environ Child Health
1972; 18:217-24
[32] Fakhir S, Ahmad P, Faridi MA, Rattan A.
Cell-Mediated immune
responses in malnourished host. J. Trop. Pediatr 1989;
35:175-8
[33] Zeng B, Qian Y, Zheng D, Wu K, Zhou M, Gong Q.
Change of T
lymphocyte subsets in peripheral blood of children with
malnutrition and
zinc deficiency. Hua His. I Ko. Ta. Hsueh Pao 1991;
22:337-9
[34] Gernaat HB, Dechering WH,Voorhoeve HW. Mortality
in severe
protein-energy malnutrition at Nchelenge Zambia. J Trop.
Pediatr 1998;
44:211-7
[35] Sheikh MM, Ansari Z, Ahmad P, Tyagi SP.
Tuberculous
lymphadenopathy in children. Indian Pediatrics 1981; 18:
293-297
[36] Sibanda EN, Stanczuk G. Lymph node pathology in
Zimbabwe: a
review of 2194 specimens. Q. J. Med. 1993; 86:811-7
[37] Fawzi WW, Msamanga GI, Spiegelman D, et al.
Randomized trial
effects of vitamin supplements on pregnancy outcomes and
T cell counts in
HIV-1-infected women in Tanzania. The Lancet 1998;
351:1447-1482
Competing interests: No competing interests
Aids, Covid and the same blunders all over again ex The Conservative Woman
by
Neville Hodgkinson
QUOTE
IN common with many others, I have been uneasy from the start over the way
Covid-19 has been handled by governments and the mainstream media. It seemed
that only one narrative was permitted – extreme fear, to be encouraged through
lockdowns, masks and exaggerated, cumulative, endlessly repeated statistics on
cases and deaths – and that our only way of becoming free would be for
scientists to vaccinate the world.
It is now known of course that lockdowns have proved deeply damaging, both socially and financially. In the UK, they have left us with one of the highest Covid death rates in the world, and a taxpayer bill for countless billions of pounds.
Recent ‘jab jingoism’ – claims of national superiority in our vaccine roll-out and the ridiculing of our European neighbours’ caution over possible dangers – is a cause for further alarm. Everyone hopes the vaccine will work, but it remains experimental, and its ability to block transmission is unproven.
As a veteran science and medical correspondent, I have seen previously how the world of science and its followers in media and government can lose their heads in a kind of shared psychosis when facing a major new medical challenge.
I am sorry to say that for a few years I too subscribed to a global hysteria, in the 1980s, which had us believing that every sexually active person on the planet was at risk of catching HIV and dying from AIDS.
By the early 90s, it became clear that this was simply not true, and I began to report the views of scientists who questioned the validity of various aspects of the HIV theory – the models that predicted general heterosexual spread, the test kits, reliance on the highly toxic antiviral drug AZT, the search for a vaccine, even the very existence of the virus as a genuine disease entity as opposed to an endogenous signal of an already compromised immune system.
I was working under an editor (Andrew Neil at the Sunday Times) who welcomed challenges to orthodoxy as long as they were evidence-based. Lacking the power to answer the questions we were raising, the journal Nature instituted a campaign of ridicule. Nature’s editor, the late John Maddox, even contemplated picketing Sunday Times offices. His campaign was supported enthusiastically by the BBC, and by the Observer and Independent (both of whose circulations had been hammered almost into oblivion by Murdoch’s Times newspapers).
It took 25 years before the World Health Organisation finally admitted there was no general heterosexual spread, and HIV was no longer deemed a ‘communicable disease of public health significance’ by US health and immigration authorities.
Money plays a part in sustaining such illusions. HIV/Aids brought hundreds of billions of dollars for research and treatment, much of it dispensed by Anthony Fauci, who still heads the US National Institute of Allergy and Infectious Diseases. It provided a gravy train for countless researchers, well-intentioned NGOs and the science journals themselves. But the cash was conditional on subscribing to the core belief, ‘HIV is the cause of Aids’. Scientists, doctors and politicians who questioned this faith and proposed or implemented non-HIV treatments were ruthlessly defunded and disempowered.
I see much the same happening today with Covid, though thanks to the internet there is at least more scope for different voices to be heard.
SARS-COV-2 differs from ‘HIV’ in being a genuine viral pathogen, but victims of Covid-19 and Aids share risk factors, including poverty, malnutrition, genetic inheritance and lifestyle, which predispose to immune deficiency. Failure to take such factors into account was and is the core mistake in Aids, and is the core mistake in the response to Covid-19 today. It has caused neglect of focused care for the poor and elderly, and futile disruption in the lives of children and young people, most of whom are at minimal risk.
Nutritional support, the cost of which would be a tiny fraction of the Covid billions spent elsewhere, is a key area of neglect.
In Ireland, more than 100 doctors, scientists and academics have signed an open letter calling on their government to recommend a daily dose of 20 to 25 micrograms of vitamin D for every adult as a preventive and treatment for the disease. They also want the government to provide vitamin D supplements to vulnerable groups such as front-line health workers, older adults, and those with pre-existing conditions such as diabetes and high blood pressure.
Dr Daniel McCartney, programme director of human nutrition and dietetics at the Technological University of Dublin and Trinity College Dublin, told the Irish Examiner: ‘We were aware of ongoing research that seemed to show vitamin D played a role in protecting people against becoming seriously ill with Covid-19 and could also be used to treat people once they did become ill. We felt it to be a professional, moral and ethical imperative to act.
‘Ireland has lost more than 4,000 people to the pandemic to date. At this time of crisis, we have nothing to lose and everything to gain if we make this harmless intervention. It’s safe, cheap, and easily available.’
Elsewhere, McCartney has said evidence linking low vitamin D levels and risk of Covid-19 infection is now considerable. It includes studies which show a 25- to 30-fold reduced risk of admission to intensive care, and a substantial reduction of risk of death, in older Covid-19 patients supplemented with the vitamin.
NHS guidelines, however, remain largely dismissive, stating that there is no evidence that vitamin D helps in the prevention or treatment of Covid-19, whilst acknowledging that supplements may be needed daily in winter for healthy bones and muscle.
Lack of evidence of benefit did not stop the UK government from launching lockdowns, nor from buying millions of doses of experimental Covid vaccines. The problem is that as with ‘HIV’/Aids, once a particular treatment strategy is in place it can take years before any others get a look in.
A similar story surrounds vitamin C. Patrick Holford, who has worked for 35 years in the field of optimum nutrition, feels so strongly about C’s preventive and therapeutic potential that he has started a campaign, www.vitaminc4covid.com, petitioning governments and doctors to promote its use as well as fund further studies.
The petition states: ‘Vitamin C is a safe, inexpensive and highly effective anti-viral nutrient in the right amount, both for prevention of colds, reducing duration and severity, and for the treatment of Covid-19 in the acute phase with life-saving potential. Yet it is classified as “false information”, not recommended by governments and rarely prescribed by doctors. This has to change . . . We stand for public health and healthcare policy to be based on science with the aim of saving lives.’
Holford is main author of a review citing 117 studies relevant to these claims, published last December in Nutrients, a Swiss-based, peer-reviewed, open-access journal. His co-authors include Professor David Smith of Oxford University’s Department of Pharmacology.
He says that since that appeared, seven Covid-specific trials have been published, three of which show vitamin C levels to be vastly depleted in serious Covid-19 cases, often to the level seen in scurvy, and predictive of risk of death. Two of the trials showed an 80 per cent reduction in mortality in patients critically ill with Covid who were treated with vitamin C compared with standard therapy.
‘These results are actually better than steroids, or any drug on offer, yet are simply ignored,’ he tells me. ‘Our team of world-leading vitamin C experts, professors, doctors and nutritionists have been supplying Public Health England, the Scientific Advisory Committee on Nutrition, the National Institute for Health and Care Excellence (Nice) and the New and Emerging Respiratory Virus Threats Advisory Group (Nervtag) with all this evidence but they just don’t respond. This ignoring of the evidence has been going on for almost a year.
‘Much like vitamin D, there is no scientific, ethical or practical reason to simply ignore the fact that these nutrients, if used in the right amounts at the right time, would immediately save lives with no risk and minimal cost.’
I learned recently that the original Hippocratic oath for doctors does not say ‘First do no harm’, but states: ‘I will use those dietary regimens which will benefit my patients according to my greatest ability and judgment, and I will do no harm or injustice to them. Neither will I administer a poison to anybody when asked to do so.’
Erm, excuse me: far from using ‘dietary regimens which will benefit’, the global response to Covid-19 has put 6.7million children at risk of being severely malnourished, according to Unicef. In the US, an unprecedented 14million children are going hungry due to the economic fallout, nearly three times the number who went hungry during the 1930s recession. About 2.5million people have died already of malnutrition and disease as a result of the restrictions, according to an analysis published last month by Swedish researchers.
It astounds me that in the UK the only effective opposition to our
Government’s participation in this psychotic episode is coming from Conservative
MPs. Why is Labour, traditionally more the party of compassion than pragmatism,
so silent? Please, will someone out there start to listen?
UNQUOTE
Believe the media? No! Not without asking questions. Learn to
Deconstruct the motives,
Read between the lines. Then think for yourself.
Oh well, forget that then.
Covid-19 Computer Models Versus Reality
QUOTE
AS WE pass through the anniversary of the week in which our freedoms
became circumscribed by the outputs of a physicist’s dodgy computer
model, Phillip W Magness at the American Institute for Economic Research
has revisited Imperial
College London’s infamous Report
9 to remind us quite how wrong it was.
He writes: ‘Ferguson’s model presented a range of scenarios under increasingly restrictive nonpharmaceutical interventions (NPIs). Under its “worst case” or “do nothing” model, 2.2million Americans would die, as would 510,000 people in Great Britain, with the peak daily death rate hitting somewhere around late May or June. At the same time, the ICL team promised salvation from the coronavirus if only governments would listen to and adopt its technocratic recommendations. Time was of the essence to act, so President Donald Trump and UK Prime Minister Boris Johnson both listened. And so began the first year of “two weeks to flatten the curve”.
‘It took a little over a month before we saw conclusive evidence that something was greatly amiss with the ICL model’s underlying assumptions. A team of researchers from Uppsala University in Sweden adapted Ferguson’s work to their country and ran the projections, getting similarly catastrophic results. Over 90,000 people would die by summer from Covid-19 if Sweden did not enter immediate lockdown. Sweden never locked down though. By May 2020 it was clear that the Uppsala adaptation of ICL’s model was off by an order of magnitude. A year later, Sweden has fared no worse than the average European lockdown country, and significantly better than the UK, which acted on Ferguson’s advice.
‘Pressed on this unexpected result, ICL tried to distance itself from the Swedish adaptation of its model in May. The records from the March 21 supercomputer run of the Uppsala team’s projections belie that assertion, linking directly to Ferguson’s March 16 report as the framework for its modelling design. But no matter – the ICL team’s own publications would soon succumb to a real-time testing against actual data.
‘A second ICL report, attempting to model the reopening of the United States from lockdowns, wildly exaggerated the death tolls that were expected to follow. By July, this model too had failed to even minimally correspond to observed reality. ICL attempted to save face by publishing an absurd exercise in circular reasoning in the journal Nature where they invoked the unrealised projections of their own model to supposedly “prove” multiple millions of lives had been saved by the lockdowns. That study soon failed basic robustness checks when the ICL team’s suite of models were applied to different geographies.
‘Another team of Swedish researchers then noticed oddities in the ICL team’s coding, suggesting they had modified a key line to bring data from their own comparative analysis of Sweden into sync with other European countries under lockdown after the models did not align. A published derivative of this discovery showed that ICL’s own attempts to validate the effectiveness of its lockdown strategies does not withstand empirical scrutiny.
‘Finally, in November, another team of researchers from the United States compared a related ICL team model for a broader swath of countries against five other international models of the pandemic, examining the performance of each against observed deaths. Their results contain a stunning indictment: “The Imperial model had larger errors, about 5-fold higher than other models by six weeks. This appears to be largely driven by the aforementioned tendency to overestimate mortality.”
‘The verdict is in. Imperial College’s Covid-19 modelling has an abysmal track record – a characteristic it unfortunately shares with Ferguson’s prior attempts to model mad cow disease, swine flu, avian flu, and countless other pathogens.’
Not only did Ferguson’s modelling overstate mortality in the absence of restrictions, it also grossly exaggerated the effectiveness of restrictions in reducing deaths.
Here are the report’s projections for the different scenarios:
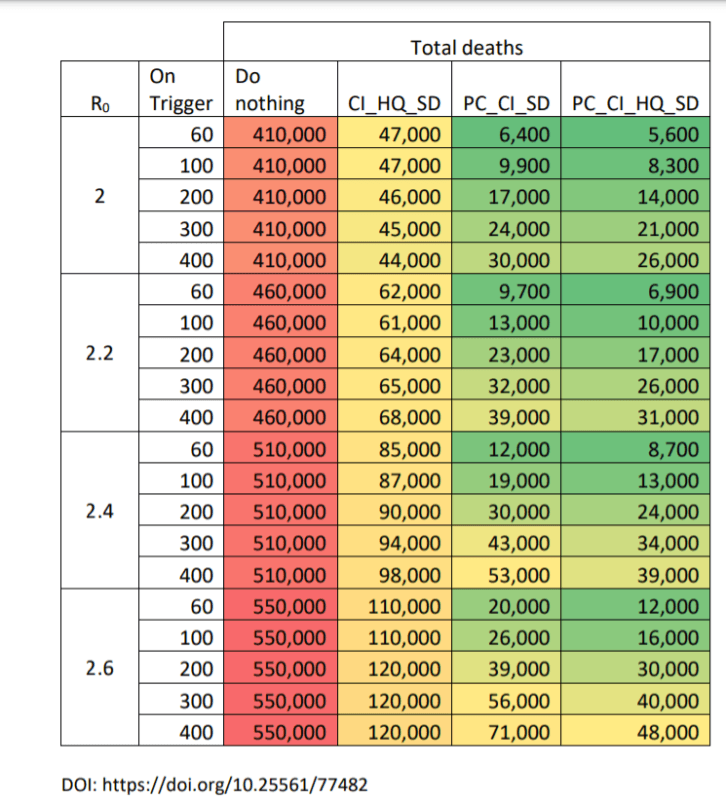
Death toll projections for different scenarios from Imperial College
Report 9
These projections for deaths in the presence of strong restrictions were
far too low – and it’s worth recalling that the Imperial team went public in
the first week of lockdown in March 2020 to predict just
5,700 UK Covid deaths in the spring under the restrictions imposed at the
time. The actual spring death toll was around 40,000.
Phillip writes: ‘As of the one-year anniversary, the UK had a little over 125,000 confirmed Covid-19 deaths. By implication, the UK death toll has exceeded the mildest of the other three NPI scenarios from the ICL model (column 2) and blown past its heavier NPI recommendations (columns 3 and 4), even while operating under a more stringent set of lockdowns than ICL originally contemplated.
‘The implications are clear. While Ferguson wildly exaggerated the “worst case” scenario for the UK, he also severely overestimated the effectiveness of NPIs at controlling the pandemic.
‘By building its policy response around the Imperial College model, the UK Government delivered the worst of both worlds. It imposed some of the most severe and long-lasting lockdowns in the world based on the premise that NPIs would work as Ferguson’s team predicted, and that such actions were needed to avert a catastrophe. Except the lockdowns did not work as intended, and the UK also ended up with an abnormally high death count compared to other countries – including locales that did not lock down, or that reopened earlier and for longer periods than the UK.’
Why is Ferguson’s Covid modelling so poor? Phillip suggests two reasons. First, as Ferguson himself made clear in his 2006 flu model on which the Covid model was based, it does not properly take into account spread in ‘residential institutions (for example, care homes, prisons) and health care settings’. When 40 per cent of deaths are care home residents and up to two-thirds of infections leading to serious illness are contracted in hospital, this is a major omission.
Second, it exaggerates the impact of restrictions on community transmission, seeming to pluck the assumptions about how much each intervention would reduce spread out of thin air. With good reason, this form of analysis was dismissed by the WHO in 2019 as not offering a reliable basis for public health policy. Phillip writes:
‘A 2019 report by the World Health Organization (WHO) warned of the flimsy empirical basis for epidemiology models such as the one developed by ICL. “Simulation models provide a weak level of evidence,” the report noted, and lacked randomised controlled trials to test their assumptions. The same report designated mass quarantine measures – what we now call lockdowns – as “Not Recommended” due to lack of evidence for their effectiveness. Summarising this literature, which included the same 2006 influenza model that Ferguson adapted to Covid-19, the WHO concluded: “Most of the currently available evidence on the effectiveness of quarantine on influenza control was drawn from simulation studies, which have a low strength of evidence”.’
As I have written before, it is admittedly counterintuitive that restrictions do not limit the spread and death toll of coronavirus in the way Ferguson and co expected. However, the data are clear that they do not, with countries and states with fewer or no restrictions frequently outperforming countries and states with some of the most strict. Since asymptomatic carriers are (despite common claims) barely infectious and account for a negligible proportion of spread, we must assume that community transmission is being driven primarily by symptomatic people who are not currently self-isolating – perhaps because they cannot, or cannot afford to, or because they think it is just a mild cold. Since even in a lockdown around half the workforce are travelling to work while only around a third work exclusively from home, many people still use supermarkets and other shops, and many children still attend school (even where the schools are open only for key workers’ children), there’s still plenty of opportunity to spread the virus.
Whatever the explanation, though, the data are unambiguous, and they do not validate Imperial’s modelling, either in terms of how many would die without restrictions or how few would die with them.
The trouble is that the assumptions behind the modelling – that lockdowns control the virus and without them hundreds of thousands more would die – have become accepted truth, to the point that journalists will just state it in their reporting as though it is undisputed fact, and politicians will instinctively impose or tighten restrictions as soon as positive cases start to rise with little or no opposition.
But you cannot ignore reality for ever. At some point something has to
give. Any day now . . .
UNQUOTE
Right or wrong?
1 In 3 Americans Think Fauci Putting Big Pharma Above Interests of Americans
[ 9 April 2021 ]
QUOTE
A new poll reveals that 32 percent of Americans feel Dr.
Anthony Fauci is
prioritizing the interests of the pharmaceutical industry over the American
public.
The poll was conducted by John Zogby Strategies and found that 31.7 percent of adults polled felt that Dr. Fauci “has the pharmaceutical industry’s best interest at heart” and just 44.9 percent felt that he “has the public’s best interest at heart.”
23.4. percent of U.S. adults polled were “not sure” who Fauci – the
federal
government’s highest-paid employee – was prioritizing.
UNQUOTE
Fauci is a wrong 'un or is he the victim of a bad press? Lotsa people don't
trust him. Nor do I.